COVID-19 Outbreaks in Co-Morbid Patients: A Pursuit for Biomarkers
-
Kaiser Jamil


Department of Genetics, Bhagwan Mahavir Medical Research Centre, 10-1-1, Bhagwan Mahavir Marg, AC Guards, Hyderabad, Telangana 500004, India
Naga ChaitanyaDepartment of Intensive Care Unit, Mahavir Hospital and Research Centre,10-1-1, Utkoor-Mogdumpur Road, AC Guards, Lakdikapul, Hyderabad, Telangana 500004, India
Shyam GadeDepartment of Head of ENT, Mahavir Hospital and Research Centre, 10-1-1, Utkoor-Mogdumpur Road, AC Guards, Lakdikapul, Hyderabad, Telangana 500004, India
M. AsimuddinDepartment of Genetics, Bhagwan Mahavir Medical Research Centre, 10-1-1, Bhagwan Mahavir Marg, AC Guards, Hyderabad, Telangana 500004, India
| Received 28 Sep, 2022 |
Accepted 15 Dec, 2022 |
Published 30 Jun, 2023 |
COVID-19 is a disease caused by SARS-CoV-2 a new coronavirus that has devastated the world economy, with its rapid spread, causing not only panic but also causing morbidity and mortality. Hence, it was declared a pandemic by WHO in 2019. Further down the lane in 2021-22, researchers and attending health officials observed that the susceptible group who were victims of the novel coronavirus were diabetics, hypertensive, or suffering from chronic obstructive pulmonary diseases or other diseases of the lungs or cancers. Furthermore, hypertension, diabetes and cardiovascular diseases were important risk factors for progression and unfavourable outcomes in COVID-19 patients. Increased expression of ACE2 was reported in diabetic, hypertensive and obese patients. The ACE2 receptor is the channel for entry of SARS-CoV-2 into the human body, but this receptor is also commonly found on the epithelial cells of several other organs such as the lungs, intestine, kidney, blood vessels and other organs enabling the entry of the coronavirus into these organs causing multiorgan failures. Thus, emphasizing the need for further studies on SARS-CoV-2-specific complications in comorbid patients and the need to identify biomarkers for the onset of the diseases. Interestingly, age is independently not a risk factor as there are reports that besides seniors and elderly people, others in their teens or twenties may develop a severe form of the disease, may require intensive care and may die as well. Hence, inflammatory conditions as evidenced by elevated levels of biomarkers like TNF-alpha, IL-6, cytokine antagonists, etc., could be investigated further to elucidate the mechanism of inflammatory response due to virus infection. Moreover, due to insufficient genetic data, the phenomena of coronavirus S-protein binding towards ACE2 in several organs is still a mystery. Hence, this article attempts to review the etiology and pathophysiology and current scenario of biomarkers for SARS-CoV-2 infections, to identify a panel of biomarkers.
INTRODUCTION
Current scenario of SARS-CoV-2 infections: The Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2), is a single-stranded RNA virus and is the cause of the ongoing COVID-19 disease1.
Published studies and WHO reports observed that within a span of about 200 days of its start, this highly infectious novel coronavirus caused 761780 deaths globally and the death toll continued to increase dramatically on a daily basis2,3.
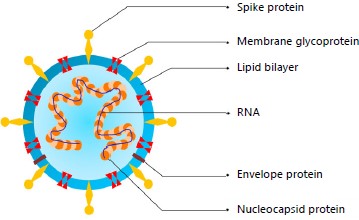
The fight against the COVID-19 pandemic has required unprecedented efforts by the research community to understand, diagnose and treat the SARS-CoV-2 virus4. The global case count (as of March 10, 2022) was 451,936,914 confirmed cases, 6,024,635 deaths (1.4%). As of April 28, 2020, the COVID-19 pandemic has infiltrated over 200 countries and affected over three million confirmed people which has subsequently increased in the last year. SARS-CoV-2, belonging to the coronavirus family, was first identified in Wuhan, China and soon became a pandemic in March 2020 as declared by WHO. Despite extensive efforts by governments, healthcare services and research groups, sadly, millions have lost their lives across the globe. Presently, innumerable published articles are available on this topic, yet there are very few critical reviews on the impacts of COVID-19 and its implications in comorbid patients5. But the understanding of what the virus does to the body in individuals with various chronic diseases and how the body reacts to it has uncovered a gamut of potential biomarkers, this aspect is interestingly confusing. Researchers have uncovered much about SARS-CoV-2 and made extraordinary and unprecedented progress in the development of COVID-19 vaccines, but there is still great uncertainty as the pandemic continued to evolve new variants, as new threats. Even though the basic structure of the coronavirus-19 is simple, as shown in Fig. 1, a single RNA strand in an envelope of lipid bilayer decorated with spike proteins (Fig. 1) but its implications are vast and unpredictable. Since its basic structure was decoded rapidly by Scientists and its mode of entry in the host was identified, the field of vaccine development went very fast. However, in the recent past, we have witnessed a tremendous socioeconomic impact due to lockdowns-people needing isolation, social distancing and travel restrictions. The healthcare burden of patients and the mortality of treating physicians and healthcare workers in large numbers was a complete disaster.
Virus and its implications in the host
Virus detection and symptoms caused: The spread of SARS-CoV-2 virus was shown to be through the breath, cough or sneeze of the infected person or the diseased person. The symptoms can vary from fever, runny nose, cough, difficulty breathing, tiredness, sometimes there is loss of smell and more complicated effects in comorbid patients. The single-stranded RNA virus of SARS-CoV-2 virus as described (Fig. 1) is enveloped with various structural proteins. The surface spike protein of the coronavirus binds to the receptor of Angiotensin-Converting Enzyme 2 (ACE2) present on the membrane of various human cells, allowing it to enter the host cells and then it starts to show its damaging effects in genetically susceptible individuals. However, some patients do not have any symptoms, yet they can be carriers, making the infection easier to spread.
|
The S1 subunit of the spike protein mediates attachment, as it consists of the Receptor Binding Domain (RBD) that binds to the human cellular ACE2 (hACE2) receptor, facilitating viral-host cell attachment. The S2 subunit of the spike protein facilitates membrane fusion with the host cell and the virus gains entry into the human cell to cause the disease known as COVID-19 the disease can be mild, or severe requiring a ventilator and oxygen. But, due to insufficient knowledge or the understanding of the binding process of the coronavirus S-protein to the ACE2 receptor, the phenomenon is still a mystery.
Co-morbidities and SARS-CoV-2: As COVID-19 is a relatively new disease, scanty information about its occurrence in co-morbid patients was available, hence, it was not easy to determine its risk factors as it was found to vary with age and underlying co-morbidities. Nevertheless, facts emerged that the coronavirus mostly attacked those individuals suffering from heart disease, or diabetics and those with pulmonary and lung diseases or aged people above 50 years of age. This information was further documented by several other researchers also who reported that 68% of patients with heart diseases also had at least one other ailment. Further, about 59% of patients with congenital heart disease remained at very high risk for COVID-197.
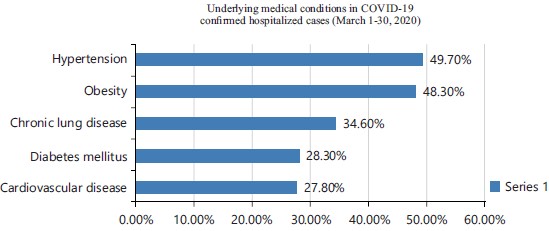
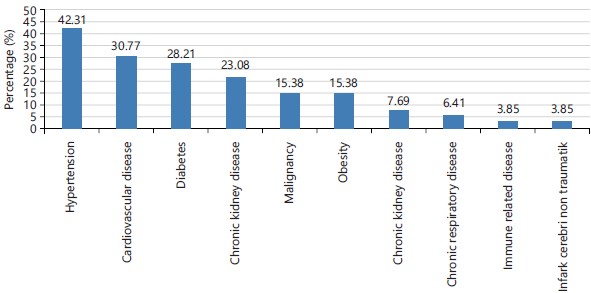
High risk patients for COVID-19 included in a study8 are mostly diabetics, hypertensive and patients with liver lung, kidney diseases and also those on chemotherapy (Fig. 2)9,10. Others who can be at risk are smokers or patients taking steroids, the morbidity and mortality of this scenario being represented in Fig. 311. It is now understood that people with comorbidities and especially with respiratory tract infections suffer from unfavourable outcomes. Among the numerous reports which emerged on COVID-19 attacks was that of dementia which occurred in patients who suffered from pneumonia, CHF, CVD, type 2 diabetes, atrial fibrillation, or those who had previous stroke12.
Detailed information on the causality and mechanism of death, as well as the spectrum of comorbidities in cases with the fatal outcome will allow accurate assessment of the hazardous nature of COVID-19 yet is missing. This could be due to one of the factors that there is this vast presence of ACE2 receptors which are not only present in the lung epithelium but also found in other organs such as the heart, liver, kidney, pancreas, small intestine and also the central Nervous system and as we know SARS-CoV-2 viruses gain entry in the cells through the ACE2 receptor.
Another interesting and factual study showed that multi-organ failure was the most common cause of death in COVID-19 patients due to pulmonary associated diseases like pneumonia as SARS-CoV-2 causes alveolar damage the cause of death could be immediate. These authors Elezkurtaj et al.13 further demonstrated that patients with comorbidities were at very high risk for mortality. Hence, deciding the causes of death in such complicated cases has been as tough as the mechanism of death could be due to their pre-existing conditions or related to COVID-19 or both. The cause of death among COVID-19 patients was found to be highest in elderly patients as many of them suffered from comorbidities and were more susceptible to the coronaviruses14,15. Hence, it became evident that the patients with low immunity, or with many combined diseases suffered with incurable consequences and death. Hence, the quest for more research specially on the discovery of novel biomarkers is most essential.
Biomarkers-definition, types, role in pathophysiology: The understanding of the pathophysiology of COVID-19 disease is believed to help in the search for the biomarkers for SARS-CoV-2. To date, there is no efficient biomarker for the timely prediction of disease progression in patients. To analyze the inflammatory profiles of COVID-19 patients and demonstrate their implications for the illness and progression of the disease, biopsy samples are required, which are not available to most researchers, this has hampered research in this direction. Further, advanced technology platforms and sophisticated lab equipment are required when performing research involving biomarkers, drug targets, cytokines and receptors, viral proteins and their related monoclonal antibodies, as well as cDNA clones. Biomarkers for COVID-19 can be very useful and important to clinicians in assessing the patients to decide the treatment strategy for close monitoring.
|
|
Further, biomarkers can be prognostic, or diagnostic and can help in improving the outcomes and also help in categorizing the patients into sub-groups such as severe, mild, or chronic16. For example, troponin biomarker levels differed in different patients and could be categorized for treatment options in COVID-19 cases, severity in cases were admitted to ICU and these patients had onset of ARDS. Variability in similar cases could be due to inter-individual variability and also could be accounted to the differences in patients’ exposure period to the virus. The levels of biomarkers may change according to the severity of COVID-19 infections17. As the virus (SARS-CoV-2) primarily targets the human lung epithelial cells, hence some authors have suggested that Linoleic acid, a Polyunsaturated Fatty Acid (PUFA), which has demonstrated efficacy against SARS-CoV-2 by inhibiting viral entry and possibly preventing infection in the human cells, can be used as a predictive biomarker for COVID-19 disease18.
Genetic study gives extensive insights into severe COVID-19: In a recent publication Nature (Journal) has reported about 16 new genetic variants, all these variants were related to the biochemical functions in the diseased patients such as immuno compromised, thromboses, swollen and painful conditions.
These discoveries can be the tip of the iceberg, to start of a new beginnings in the search of biomarkers for early detection of the diseases like COVID-19. This study further observes that the genes responsible for the bleeding disorders in COVID-19 cases control the levels Factor VII and can cause excessive nose bleeds(epitaxis) or excessive bleeding after surgery. Thus, clotting abnormalities in COVID-19 patients may be due to mutations in the F-7 genes19.
Clinical biomarkers are generally defined as the measurable biological indicators of the presence, severity or type of disease in medical settings. Biomarkers can be applied to describe observable characteristics of a certain disease and to determine optimal treatments based on these phenotypes, as well as genotypes, thence, they have received substantial attention. In particular, respiratory disease biomarkers, such as those associated with Acute Respiratory Distress Syndrome (ARDS), have been associated with increased mortality (IL-8, ICAM-1) and improved survival (nitric oxide). These biomarkers play a pivotal role in predicting future complications or severity of disease and could be useful as an indicator for COVID-19 prognosis. The answer to all the COVID-19 patients with co-morbidities is entirely due to the presence of ACE2 receptors found in organs other than lungs only. To prevent fatal outcomes-it is important to discover biomarkers for early detection. Biomarkers can be of the following types: Biomarkers of disease progression, haematological biomarkers, immunological biomarkers, inflammatory biomarkers, Neutrophil-Lymphocyte Ratio (NLR). Hence this study tries to present the pathophysiology and continues to search for the biomarkers for SARS-CoV-2.
Biomarkers identified/possible biomarkers for COVID-19: It has recently emerged that COVID-19 is not a single disease related to the coronavirus, but a combination of diseases related to age and also to other comorbidities. In such a scenario, biomarkers can play a vital role in the early detection, diagnosing and monitoring the patients for their complicated health issues. This could also benefit the attending Health care providers to manage and monitor the patients. Biomarkers have the advantage of predicting the patients’ risk conditions and aid in preventing drastic consequences in patient care. The importance of biomarkers is evident, hence, the need to include them in clinical settings. Because of the heterogeneity of COVID-19 disease due to comorbidity a panel of biomarkers rather than a single biomarker may provide more useful information.
Literature has led us to identify several biomarkers in at least thirty-four articles, these are summarised as follows: Biochemical biomarkers include-lactate dehydrogenase, cardiac troponin, renal proteins, among serum biomarkers-c-reactive proteins and serum amyloid A, showed higher levels in patients compared to controls. Besides these, there was a significant increase in lymphocyte and platelet count and also an increase in neutrophil to lymphocyte ratio, D-dimer and interleukin-6, however, this is not an exhaustive list. Nonetheless, such biochemical medical records give the Clinicians a tool to modify the treatment strategy of the patients, so they could stratify the patients into sub-groups for targeted therapy. Other authors included white cell count, C-reactive proteins, LDH, CRP and TNF-alpha.
Inflammatory conditions as evidenced by elevated levels of TNF-alpha, IL-6, cytokine antagonists, etc., could be investigated further to elucidate the mechanism of inflammatory response due to virus infection.
Several studies have shown that patients infected with SARS-CoV-2 showed high levels of pro-inflammatory cytokines including IL-1, IL-2, IL-6, IL8, IL-17, G-CSF, GM-CSF and chemokines such as IP-10 and MCP-1 in the sera during the disease and may play a key role in the development of lung dysfunction by leading to the accumulation of immune cells within the lungs20. Hence, IL6 can be regarded as a potential biomarker of SARS-CoV-2, as increased concentrations of IL-6 were reported to be associated with increased viral load and this leads to the recruitment of inflammatory monocytes for countering the attack. The Suppressor of Cytokine Signalling 3 (SOCS3) regulates the negative feedback mechanism of IL-6, which is found to be reduced in patients with COVID-1921,22. Plasma TNF-α was also reported to be moderately regulated in SARS-CoV-2 patients. Further haematological biomarkers can also be considered key factors for predicting severe COVID-19 outcomes23. Reports from developing countries suggest that liver function tests could predict the severity of COVID-1924.
All biomarkers are generally quantitative measurements used clinically for many conditions reflecting pathological development. Researchers are trying to understand why some people never get COVID-19, even if they’ve been exposed to the virus. In trying to answer such questions we turn to look at the fact of genetic susceptibility and genetic resistance. Some will simply allocate this to our immune system, which in turn is controlled by genes. Since the beginning of the pandemic, researchers have been mapping the virus spike and Angiotensin-Converting Enzyme 2 (ACE2) binding sites to determine the structural basis of recognition. Infections of the SARS-CoV-2 viruses cause multi-organ failures in co-morbid patients25.
Samprathi and Jayashree26 have demonstrated a whole spectrum of biomarkers for various stages of COVID-19 diseases, such as their role in patient management, biomarkers affecting various organs of the body, Sequential course of biomarkers and how each biomarker have an independent role depending on the organ and stage of the disease. This enormous data could be difficult for physicians to consolidate and analyse for patient benefit. Using this information, Scientists have been able to identify several potential inhibitors, including Human Monoclonal Antibodies (mAbs), Single-Domain Antibodies (nanobodies) and nanoparticles. Inflammatory conditions as evidenced by elevated levels of TNF-alpha, IL-6, cytokine antagonists, etc, as described earlier and these could be investigated further to elucidate the mechanism of inflammatory response due to virus infection.
Finally, this article has certain limitations. It was limited to a certain period and only included studies published since the origin of COVID-19 (since 2019 only). We find that there is a lack of research on identifying risk factors in comorbid patients. The COVID-19 pandemic is a scientific, medical and social challenge. Individuals with pre-existing illnesses or chronic diseases or age-related seniors or obese patients were at increased risk of developing COVID-19. Also, their causes of death were not established systematically due to the prevailing non-autopsy situation during the pandemic. Furthermore, this article endorses the importance of clinical autopsies for a full understanding of the actual death of the patients. To determine the severity of COVID-19 disease development, an understanding of the dysregulation of the immune system is vital.
CONCLUSION
Highest mortality in COVID-19 cases could be related to the co-morbid conditions, the most common comorbid conditions include heart diseases or diabetes. More than half of the patients had two or more comorbidities. The biomarker research on COVID-19 is still expanding, as validation poses a great challenge. The world is likely to have many more years of COVID-19 decision-making ahead as there is no magic solution available at present. For the present we agree to the entire list of biomarkers listed in this article, however research must continue to identify novel predictive and diagnostic biomarkers for patient care and for clinicians to decide targeted therapy. This can be done by taking the comorbid conditions of patients into account. The decisions of global agencies and governments, as well as the behaviors: of citizens in every society and every country, will greatly affect the biomarker discovery ahead.
SIGNIFICANCE STATEMENT
This study is based on the fact that SARS-CoV-2 has a broad spectrum of clinical manifestations, with a high capacity of mutations, hence, it is essential to accelerated research to understand biomarkers of the disease to develop prevention, diagnosis and treatment strategies against the pandemic. Biomarkers can predict the immune response associated with infection and how they correlate with disease severity. This article throws light on the fact that the pandemic due to SARS-CoV-2 is owing to a host of confounding factors which have been identified during the early days of COVID-19 outcomes. But the need to direct research on identifying pathological mechanisms to detect the disease conditions at early stages was not challenged. Hence the need to systematically segregate the patients on the basis of their comorbid conditions has been essential, which has been attempted in this article further we discussed a diversity of genetic and protein biomarkers. COVID-19 being unpredictive and weirdest disease which we face, hence expanding our research into newer fields of predictive, prognostic and diagnostic areas may benefit the society and the world at large by pursuing novel biomarkers.
ACKNOWLEDGMENTS
We acknowledge all the sources of information included in this article. These permissions are granted for free by Elsevier for as long as the COVID-19 Resource Centre remains active. Permissions from NIH and other journals are also granted. We thank, the Chairman and Research Director of Mahavir Hospital and Research Centre for their encouragement and support.
REFERENCES
- Jamil, K., K.K. Kakarala and M. Asimuddin, 2021. Replication of SARS CoV2 in pancreatic cells via ACE2 cell surface receptors. Madridge J. Case Rep. Stud., 5: 182-186.
- Fang L, G. Karakiulakis and M. Roth, 2020. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir. Med., 8: e21.
- Albini, A., G. Di Guardo, D.M. Noonan and M. Lombardo, 2020. The SARS-CoV-2 receptor, ACE-2, is expressed on many different cell types: Implications for ACE-inhibitor- and angiotensin II receptor blocker-based cardiovascular therapies. Intern. Emerg. Med., 15: 759-766.
- Al-Benna, S., 2020. Association of high level gene expression of ACE2 in adipose tissue with mortality of COVID-19 infection in obese patients. Obesity Med., 19: 100283.
- Jamil, K., K.K. Kakarala and R. Maturi, 2021. Outbreaks of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) in comorbid patients. Appl. Med. Res., 8.
- Muralidar, S., S.V. Ambi, S. Sekaran and U.M. Krishnan, 2020. The emergence of COVID-19 as a global pandemic: Understanding the epidemiology, immune response and potential therapeutic targets of SARS-CoV-2. Biochimie, 179: 85-100.
- Bajgain, K.T., S. Badal, B.B. Bajgain and M.J. Santana, 2021. Prevalence of comorbidities among individuals with COVID-19: A rapid review of current literature. Am. J. Infect. Control, 49: 238-246.
- Ji, W., G. Bishnu, Z. Cai and X. Shen, 2020. Analysis clinical features of COVID-19 infection in secondary epidemic area and report potential biomarkers in evaluation. medRxiv.
- Sanyaolu, A., C. Okorie, A. Marinkovic, R. Patidar and K. Younis et al., 2020. Comorbidity and its impact on patients with COVID-19. SN Compr. Clin. Med., 2: 1069-1076.
- Garg, S., L. Kim, M. Whitaker, A. O’Halloran and C. Cummings et al., 2020. Hospitalization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019-COVID-NET, 14 States, March 1-30, 2020. Centers Dis. Control Prev.: Morbidity Mortality Wkly Rep., 69: 458-464.
- Djaharuddin, I., S. Munawwarah, A. Nurulita, M. Ilyas, N.A. Tabri and N. Lihawa, 2021. Comorbidities and mortality in COVID-19 patients. Gaceta Sanitaria, 35: S530-S532.
- Qureshi, A.I., W.I. Baskett, W. Huang, S.H. Naqvi and C.R. Shyu, 2022. New-onset dementia among survivors of pneumonia associated with severe acute respiratory syndrome coronavirus 2 infection. Open Forum Infect. Dis., 9.
- Elezkurtaj, S., S. Greuel, J. Ihlow, E.G. Michaelis and P. Bischoff et al., 2021. Causes of death and comorbidities in hospitalized patients with COVID-19. Sci. Rep., 11: 4263.
- Grasselli, G., A. Zangrillo, A. Zanella, M. Antonelli, L. Cabrini and A. Castelli et al., 2020. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA., 323: 1574-1581.
- Onder, G., G. Rezza and S. Brusaferro, 2020. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA, 323: 1775-1776.
- Chen, C.H., S.W. Lin, C.F. Shen, K.S. Hsieh and C.M. Cheng, 2022. Biomarkers during COVID-19: Mechanisms of change and implications for patient outcomes. Diagnostics, 12: 509.
- Kermali, M., R.K. Khalsa, K. Pillai, Z. Ismail and A. Harky, 2020. The role of biomarkers in diagnosis of COVID-19-A systematic review. Life Sci., 254: 117788.
- Valdés, A., L.O. Moreno, S.R. Rello, A. Orduña, D. Bernardo and A. Cifuentes, 2022. Metabolomics study of COVID-19 patients in four different clinical stages. Sci. Rep., 12: 1650.
- Kousathanas, A., E. Pairo-Castineira, K. Rawlik, A. Stuckey and C.A. Odhams et al., 2022. Whole-genome sequencing reveals host factors underlying critical COVID-19. Nature, 607: 97-103
- Iwamura, A.P.D., M.R.T. da Silva, A.L. Hümmelgen, P.V.S. Pereira and A. Falcai et al., 2021. Immunity and inflammatory biomarkers in COVID-19: A systematic review. Rev. Med. Virol., 31.
- Liu, F., L. Li, M. Xu, J. Wu and D. Luo et al., 2020. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. J. Clin. Virol., 127: 104370.
- Liu, T., J. Zhang, Y. Yang, H. Ma and Z. Li et al., 2020. The role of interleukin‐6 in monitoring severe case of coronavirus disease 2019. EMBO Mol. Med., 2: e124211.
- Ponti, G., M. Maccaferri, C. Ruini, A. Tomasi and T. Ozben, 2020. Biomarkers associated with COVID-19 disease progression. Crit. Rev. Clin. Lab. Sci., 57: 389-399.
- Ahmed, Z., U. Ahmed, S. Walayat, J. Ren and D.K. Martin et al., 2018. Liver function tests in identifying patients with liver disease. Clin. Exp. Gastroenterol., 11: 301-307.
- Zaim, S., J.H. Chong, V. Sankaranarayanan and A. Harky, 2020. COVID-19 and multiorgan response. Curr. Probl. Cardiol., 45: 100618.
- Samprathi, M. and M. Jayashree, 2020. Biomarkers in COVID-19: An up-to-date review. Front. Pediatr., 8.
How to Cite this paper?
APA-7 Style
Jamil,
K., Chaitanya,
N., Gade,
S., Asimuddin,
M. (2023). COVID-19 Outbreaks in Co-Morbid Patients: A Pursuit for Biomarkers. Asian Journal of Emerging Research, 5(1), 1-8. https://doi.org/10.3923/ajerpk.2023.01.08
ACS Style
Jamil,
K.; Chaitanya,
N.; Gade,
S.; Asimuddin,
M. COVID-19 Outbreaks in Co-Morbid Patients: A Pursuit for Biomarkers. Asian J. Emerg. Res 2023, 5, 1-8. https://doi.org/10.3923/ajerpk.2023.01.08
AMA Style
Jamil
K, Chaitanya
N, Gade
S, Asimuddin
M. COVID-19 Outbreaks in Co-Morbid Patients: A Pursuit for Biomarkers. Asian Journal of Emerging Research. 2023; 5(1): 1-8. https://doi.org/10.3923/ajerpk.2023.01.08
Chicago/Turabian Style
Jamil, Kaiser, Naga Chaitanya, Shyam Gade, and M. Asimuddin.
2023. "COVID-19 Outbreaks in Co-Morbid Patients: A Pursuit for Biomarkers" Asian Journal of Emerging Research 5, no. 1: 1-8. https://doi.org/10.3923/ajerpk.2023.01.08

This work is licensed under a Creative Commons Attribution 4.0 International License.