The Pattern of Rickets and Rickets-Like Bone Deformities in South-West Nigeria
-
Emmanuel O. Adeniji
College of Health Sciences, Ladoke Akintola University of Technology, Osogbo, Osun State, Nigeria
Isaac O. Oluwayemi

Department of Paediatrics, Faculty of Clinical Sciences, College of Medicine, Ekiti State University, Ado-Ekiti, Ekiti state, Nigeria
Temitope O. AyeniDepartment of Paediatrics, LAUTECH Teaching Hospital, Osogbo, Osun State, Nigeria
Ayotunde E. AjibolaDepartment of Paediatrics, Ekiti State University Teaching Hospital, Ado-Ekiti, Ekiti State, Nigeria
| Received 10 Nov, 2020 |
Accepted 19 Feb, 2021 |
Published 15 Apr, 2021 |
ABSTRACTBackground and Objective: Rickets is the most common childhood metabolic disorder of bones characterized by deficient mineralization of the growth plates. The prevalence of rickets is reducing particularly in developed countries where there is routine vitamin D supplementation in infants and children but it still constitutes a significant burden in developing countries. The index study aims to provide a 10-year review of clinical rickets and ricket-like bone deformities among children in South-West Nigeria. Materials and Methods: This is a retrospective descriptive study of a total of 66 children managed for rickets and rickets like bony deformities at the Ekiti State University Teaching Hospital (EKSUTH) and LAUTECH Teaching Hospital (LTH) for 10 years. Results: Forty-eight (72.7%) were managed at EKSUTH while 18 (27.3%) were seen at LTH. Of the 66 children, there were 39 (59.1%) males and 27 (40.9%) females giving a M:F of 1.4:1. The mean age for the presentation of rickets and rickets-like bone deformities were 2.9 ± 1.68 years and 3.3 ± 2.60 years respectively. Rickets was found in 41 (62.1%) and rickets-like genu valgum in 14 (21.2%) patients which represented 56% of all rickets-like bone deformities. Conclusion: Rickets was commoner than rickets-like bone deformities in all age groups. Rickets was predominant among female children at LTH Osogbo.
INTRODUCTION
Rickets is the most common childhood metabolic disorder of bones characterized by deficient mineralization of the growth plates1,2. Globally, the commonest cause of rickets is vitamin D deficiency which is primarily supplied through direct exposure to sunlight and nutritional intake3,4. However, in Sub-Saharan Africa including Nigeria, calcium deficiency has been reported as the most prevailing cause of rickets5,6.
The prevalence of rickets is reducing particularly in developed countries where there is routine vitamin D supplementation in infants and children but it still constitutes a significant burden in the developing countries including Nigeria6. Rickets is a cause of concern majorly because it reduces the linear growth of a child with associated bony deformities of varying degrees depending on its severity. This results in physical disabilities and negatively affects the quality of life of the child if left untreated5.
The diagnosis of rickets can be made with suggestive clinical features and confirmed by elevated alkaline phosphatase and certain radiographic bony changes that are characteristic7. However, some children have bony deformities characteristic of rickets but with normal serum alkaline phosphatase and absence of characteristic features of rickets on plain radiograph, such patients are said to have Ricket-like bony deformities7.
The index study is a ten-year (March 2010 to March 2020) review of rickets and Ricket-like bone deformities among children managed at the Paediatric Endocrinology units of two State Teaching Hospitals (Ekiti State University Teaching Hospital and LAUTECH Teaching Hospital, Osun State) in South-West Nigeria.
MATERIALS AND METHODS
The index study is a retrospective descriptive study of all children managed for childhood rickets and rickets-like bone deformities at the Ekiti State University Teaching Hospital (EKSUTH) and LAUTECH Teaching Hospital (LTH) for 10 years from March 2010 to March 2020. Ethical clearance for the study was obtained from the Ethics and Research Committee of EKSUTH and LTH respectively.
Data Collection: Biodata and essential clinical information about patients seen at the endocrinology clinics of both centres were entered into an Excel spreadsheet at presentation for effective follow-up of the patients. Relevant data were extracted, entered into and analyzed with the Statistical Package for Social Sciences for Windows version 22. Patients’ ages were categorized into three (3 years and below, >3 – 5 years, and above 5 years); the frequency of rickets and rickets-like bone deformities with sex distribution in each age category was determined and charted. Rickets and rickets-like bone deformities were also compared for both EKSUTH and LTH centres. The different types of rickets-like deformities were classified as knock-knee (genu valgum), bow legs (genu varum), wind-swept deformity and malunion of fractured bone; and their frequency was determined and charted.
RESULTS
A total of 66 Children were managed for childhood rickets and rickets-like bone deformities in the two-State Teaching Hospitals (Ekiti State University Teaching Hospital, Ado-Ekiti and LAUTECH Teaching Hospital, Osogbo), between March 2010 to March 2020. Forty-eight (72.7%) were managed at EKSUTH while 18 (27.3%) were seen at LTH. Of the 66 children, there are 39 (59.1%) males and 27(40.9%) females giving a male to female ratio of 1.4:1. The mean age for the presentation of rickets was 2.9 ± 1.68 years while the mean age for the presentation of rickets-like bone deformities was 3.3 ± 2.60 years. Figure 1 showed that the majority of rickets and rickets-like deformities were found in children aged 3 years and below.
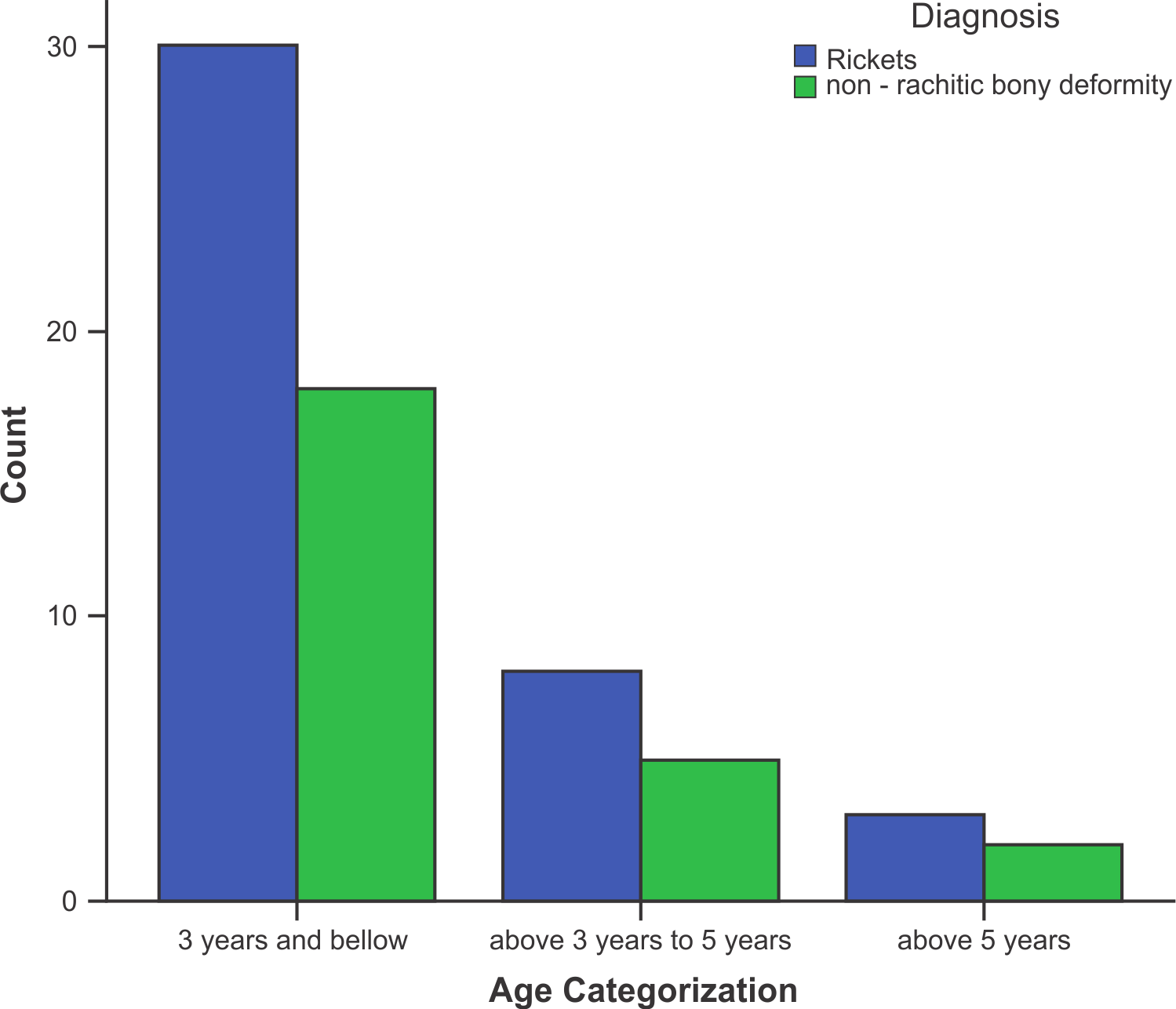
Rickets was found in 41 (62.1%) of the 66 patients, followed by rickets-like genu valgum in 14 (21.2%). Genu valgum (knock-knees) was the most common (56%) rickets-like bone deformities seen, Details of other rickets-like bony deformities are shown in Table 1.
|
|||||
| Description of Bone deformities | Frequency | Overall Percent (%) | Sub-group percent (%) | ||
| Rickets | 41 | 62.1 | |||
| Rickets-like bone deformities | |||||
| Knock-knee (genu valgum) | 14 | 21.2 | 56.0 | ||
| Bow legs (genu varum) | 9 | 13.6 | 36.0 | ||
| Wind-swept deformity | 1 | 1.5 | 4.0 | ||
| Mal-union of the previous fracture | 1 | 1.5 | 4.0 | ||
| Total | 66 | 100.0 | |||
Of the 48 patients that were managed at EKSUTH, 25 (52.1%) had rickets while the remaining 23 (47.9%) were managed for rickets-like bone deformities. Among the 18 patients managed at LTH, Osogbo, 16 (88.9%) had rickets while the remaining were cases of rickets-like bone deformities as shown in Fig.2.

Figure 3 shows the pattern of distribution of rickets and rickets-like deformities according to age group and gender in each center. At LTH 84.6% of children aged 3 years and below had rickets compared to 62.5% of the same age group at EKSUTH. Also, rickets was the only presentation in the age groups older than 3 years at LTH compared to EKSUTH where there was almost equal representation of rickets and rickets-like bone deformities. Figure 3 also showed that females are mostly affected with rickets at LTH compared to EKSUTH where males predominated.
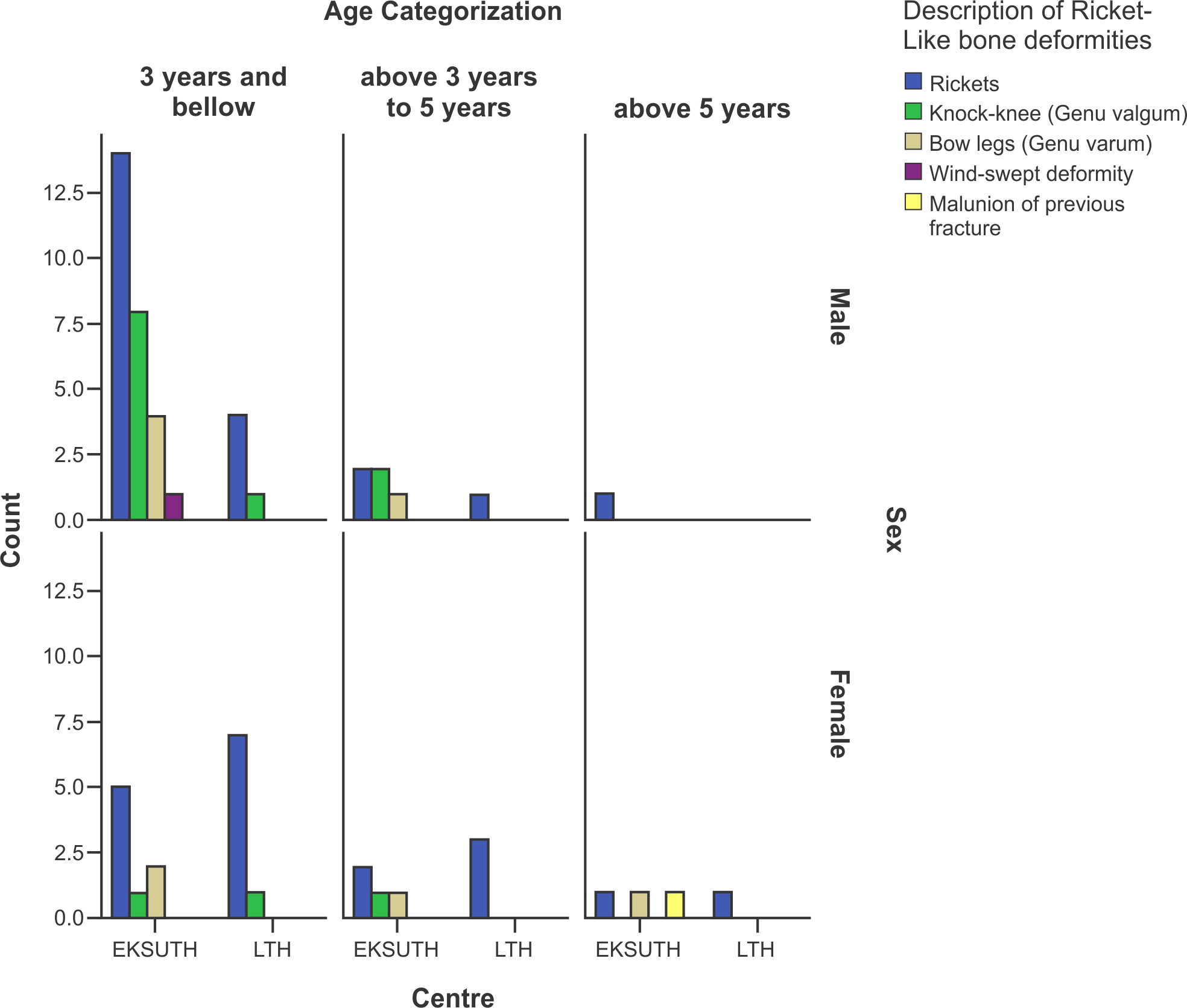 |
Figure 3: Pattern of Rickets and Ricket-like bone deformities according to age-group & sexper centre |
DISCUSSION
The occurrence of rickets is greater than that of rickets-like bone deformities in all age groups of the patients. This is similar to the finding of Fischer et al8 but contrary to the finding of Jones et al4 among Gambian children who found the majority of the children studied to have rickets-like bone deformities with few having active rickets. The Gambian study was a community-based study that involved screening of a large population of children for rickets-like bone deformities; by this, a lot of children who wouldn’t have presented to the hospital were discovered. The index study was hospital-based, and it is possible that more patients had rickets because of other non-skeletal presentations, which may be life-threatening, thereby forcing the parents to bring such children to the hospital. Examples of such presentations include seizures, pneumonia, failure to thrive, delayed developmental milestone (delayed tooth eruption and delayed walking) etc7,9.
The mean age for the presentation of rickets-like bone deformities in the patients was 3.3years. This was similar to the finding (median of 3.6 years) of Jones et al 4. The patients with active rickets had a lower mean age of 2.9years. This is expected because rickets is very likely to prevent a child from walking on time, creating anxiety in the parents which makes them bring the affected children for a medical check-up. However, children with physiologic rickets-like bone deformities are very likely to start walking at the expected age and are otherwise healthy but for the deformed limbs which when persistent beyond parents’ expectation make them present before enrollment in schools. Rickets-like bone deformities may also be a complication of rickets which had been long-standing and left unattended to until it self-corrects, however leaving the bony manifestations as a residual manifestation7,10.
Rickets was commoner in females at LTH unlike in EKSUTH where it was commoner in the males. This is possible because of the wearing of protective clothes called hijab by female children in the Muslim-dominated Osogbo. This could lead to vitamin D deficiency in them because of limited exposure to sunlight in such children10,11. Rickets can be prevented in the at-risk population by regular health education in the hospitals and places of worship and by giving multivitamins to the infants, in addition to adequate nutrition and exposure to early morning sunlight.
Genu valgum (knock-knee) is the leading form of rickets-like bony deformities in the index study. This is in agreement with other studies4,8. This is possible because of the mean age of presentation of the children which coincides with the age of highest incidence of knock-knees as a result of physiologic reasons10,12. Children with rickets-like deformities are often managed conservatively and followed up till the age of 5 years when most of the physiologic rickets-like deformities are expected to have auto-correct. Persistence of physiologic rickets-like bone deformities beyond 5 years of age is sent to orthopedic surgeons for surgical correction13.
CONCLUSION
Rickets remains a significant problem in children in developing countries with associated bony abnormalities, which may be disabling and permanent when left untreated. Further awareness is needed in society about the prevention of rickets and early presentation for the treatment of children with such problems.
ACKNOWLEDGEMNT
We wish to appreciate the nurses, resident doctors, medical record officers, laboratory scientists and other staff at EKSUTH and LTH who contributed to the effective management of the patients. The index study is self-sponsored.
REFERENCES
- Sahay, M. and R. Sahaya, 2012. Rickets-vitamin D deficiency and dependency. Ind. J. Endocrinol. Metab., 16: 164-176.
- Glorieux, F.H. and J.M. Pettifor, 2014. Vitamin d/dietary calcium deficiency rickets and pseudo-vitamin d deficiency rickets. BoneKEy Rep.
- Al-Atawi, M.S., I.A. Al-Alwan, A.N. Al-Mutair, H.M. Tamim and N.A. Al-Jurayyan, 2009. Epidemiology of nutritional rickets in children. Saudi J. Kidney Dis. Transplant., 20: 260-265.
- Jones, H.L., L. Jammeh, S. Owens, A.J. Fulford, S.E. Moore, J.M. Pettifor and A. Prentice, 2015. Prevalence of rickets-like bone deformities in rural gambian children. Bone, 77: 1-5.
- Thacher, T.D., P.R. Fisher, M.A. Strand and J.M. Pettifor, 2006. Nutritional rickets around the world: Causes and future directions. Ann. Trop. Paediatr., 26: 1-16.
- Oginni, L.M., M. Worsfold, O.A. Oyelami, C.A. Sharp, D.E. Powell and M.W.J. Davie, 1996. Etiology of rickets in Nigerian children. J. Pediatr., 128: 692-694.
- Fischer, P.R., T.D. Thacher and J.M. Pettifor, 2008. Pediatric vitamin D and calcium nutrition in developing countries. Rev. Endocr. Metab. Disord., 9: 181-192.
- Fischer, P., 1999. Nutritional rickets without vitamin D deficiency in Bangladesh. J. Trop. Pediatr., 45: 291-293.
- Julies, P., R.M. Lynn, K. Pall, M. Leoni and A. Calder et al., 2020. Nutritional rickets under 16 years: UK surveillance results. Arch. Dis. Childhood, 105: 587-592.
- Tschinkel, K. and R. Gowland, 2020. Knock-knees: Identifying genu valgum and understanding its relationship to vitamin D deficiency in 18th to 19th century northern England. Int. J. Osteoarchaeol., 30: 891-902.
- Wakayo, T., T. Belachew, H. Vatanparast and S.J. Whiting, 2015. Vitamin D deficiency and its predictors in a country with thirteen months of sunshine: the case of school children in central Ethiopia. PLoS ONE.
- Espandar, R., S.M.J. Mortazavi and T. Baghdadi, 2010. Angular deformities of the lower limb in children. Asian J. Sports Med.
- Lee, S.W., K.J. Lee, C.H. Cho, H.U. Ye and C.J. Yon et al., 2020. Affecting factors and correction ratio in genu valgum or varum treated with percutaneous epiphysiodesis using transphyseal screws. J. Clin. Med.
How to Cite this paper?
APA-7 Style
Adeniji,
E.O., Oluwayemi,
I.O., Ayeni,
T.O., Ajibola,
A.E. (2021). The Pattern of Rickets and Rickets-Like Bone Deformities in South-West Nigeria. Asian Journal of Emerging Research, 3(1), 7-11. https://doi.org/10.3923/ajerpk.2021.7.11
ACS Style
Adeniji,
E.O.; Oluwayemi,
I.O.; Ayeni,
T.O.; Ajibola,
A.E. The Pattern of Rickets and Rickets-Like Bone Deformities in South-West Nigeria. Asian J. Emerg. Res 2021, 3, 7-11. https://doi.org/10.3923/ajerpk.2021.7.11
AMA Style
Adeniji
EO, Oluwayemi
IO, Ayeni
TO, Ajibola
AE. The Pattern of Rickets and Rickets-Like Bone Deformities in South-West Nigeria. Asian Journal of Emerging Research. 2021; 3(1): 7-11. https://doi.org/10.3923/ajerpk.2021.7.11
Chicago/Turabian Style
Adeniji, Emmanuel, O., Isaac O. Oluwayemi, Temitope O. Ayeni, and Ayotunde E. Ajibola.
2021. "The Pattern of Rickets and Rickets-Like Bone Deformities in South-West Nigeria" Asian Journal of Emerging Research 3, no. 1: 7-11. https://doi.org/10.3923/ajerpk.2021.7.11

This work is licensed under a Creative Commons Attribution 4.0 International License.