Effects of ACBT with Early Mobilization on Respiratory/Hemodynamic Response of Obese ICU patients
-
Abeer Fatima

Ms-CPPT Riphah International University, Served as Lecturer in Shifa Tameer-e-Millat University
Rabbi AliMedical Officer in Shaikh Zaid Medical Hospital
Saad SharifCurrently, General Physician in Al-Azizia Medical Centre
Imran AmjadSupervisor Associate Professor/Associate Dean at Riphah College of Rehabilitation Sciences, Riphah
| Received 29 May, 2019 |
Accepted 25 Jul, 2019 |
Published 15 Aug, 2019 |
Background: Early mobilization and breathing exercises (ACBT) are used in critical care, but not enough data is available on their combined effect, especially in the obese patients in ICU, which is the focus of this study. Objectives: To determine the combined effects of Active Cycle Breathing Techniques and early mobilization on the hemodynamic and respiratory responses of Obese Patients in Intensive care unit. Materials and Methods: It is a Randomized Controlled Trial, having sample size of 58, with 29 patients in each group selected by purposive non-probability sampling technique. Study duration is 6 months. Tools used were; self-structured questionnaire, Borg’s scale, clinical Spirometer, ICU mobility scale. Data is analyzed through SPSS 20. Results: Significant improvements were noted in the respiratory parameters that is; FEV1, FVC, PEF in the experimental group (P= 0.000) along with the significant effect on some hemodynamic parameters like pulse rate and SpO2 in experimental groups (P = 0.009). Conclusion: The study concluded that there has been a positive effect of Active Cycle Breathing Technique and early mobilization combined on the respiratory and some hemodynamic responses of ill obese patients in the Intensive Care Unit.
INTRODUCTION
A strong link exists amongst the body mass index (BMI) and the disease/disabilities, especially in the chronic disease. The probability of having comorbid in obese patients increase many fold, which puts them on risk of having either prolong or frequent visits to the Intensive Care Units of the hospital1. There are many different impacts of obesity on the respiratory and hemodynamic system, like critical illness resembling those in the intensive care unit are to a great extent related to high mortality rate, which furthermore makes the sufferer more prone to having muscle weakness, physical disabilities, sleep apnea and cognitive impairments along with reduced ventilation, the airway resistance was correlated with the large BMI value2,3. As physical therapists are one of the integral part of the group or multidisciplinary team based care of the patients in Intensive care Unit, it is therefore important for them to consider holistic approach when treating the patient for their conditions therefore casual care should include the respiratory management along with the musculoskeletal and neurological care4,5.
Pakistan is a lower-middle-income country, as per The World Bank6 with the estimated population of 182.1 million, and is facing quite a higher burden of the respiratory diseases like COPD along with asthma, whereas the mortality rate due to chronic respiratory diseases is close to 138.2 per 100,000 in males and approximately 41.3 per 100,000 in females in Pakistan7. While the patients having COPD and asthma, contribute to the population of the Intensive care units in Pakistan7, therefore in order to provide effective care to these patients, physical therapist should also vigilantly fulfill their role as per patient need and requirements. One of the most troublesome event in such patients in when they are having an acute exacerbation of COPD, which means that they need critical care in such conditions and therefore have to different protocol of care under these circumstances. There are many high quality RCTs that suggest the use of Corticosteroids, early mobilization, non-invasive ventilation, antibiotic use in ICU and rehabilitation after acute exacerbation, while single high quality RCT and several low quality RCTs suggest the use of controlled oxygen therapy and breathing exercises and lastly uncontrolled trials or expert opinions are limited to the use of inhaled bronchodilators, whereas, the favored usual care consists of rehabilitation during acute exacerbation8.
Early mobilization is given with the intension of preserving of the musculoskeletal strength, improved hemodynamic and respiratory responses1. Thus counteract functional deterioration and expedite hospital discharge, in patients having high BMI and are in critical care. Breathing exercises are used to alleviate shortness of breath, increase thoraco-abdominal harmonization and augment functional capacity especially in obese patients under critical care5. Those patients who require mechanical ventilation for duration lengthier than 7 days, the occurrence of ICU acquired weaknesses increase from 25% to 60%1,9 thus these weaknesses further prolong the length of stay either in the hospital and Intensive Care Units and therefore the quality becomes compromised and further result in increased healthcare cost. Thus, as per the data, any intervention that has the ability to control these complications can positively affect the quality of life of the patient and reduce the cost of care. In this aspects Early mobilization is considered as one such intervention, which has the potential of influencing the life of the patient in appositive manner with the reduce cost. Early mobilization appears physiologically a rational method in patients who would remain immobilized, as it is a safer and feasible method, especially in obese. It helps in improving the functional recovery of the obese patients and reduces the length of hospital stay10-12.
In the previous studies on the bases of Acute Physiology & Chronic Health Evaluation II also known as (APACHE II) score of approximately 17 on the patients having a median age range of 61 found out that, the subjects had received much higher frequency of physical therapy sessions in the Intensive Care, than in the acute care wards4.
A Meta-analysis and systemic review observed the best available research evidences with respect to the volume, consistency, and generalizability of the active cycle of breathing technique (ACBT) in the Chest Physical Therapy (CPT). In this analysis, 24 studies were analyzed and there were 10 comparators identified for example; conventional CPT and PEP (positive expiratory pressure). There were different outcomes used but the most frequent was the sputum-wet weight, Forced Vital Capacity (FVC), Forced Expiratory Volume (FEV). The Standardized Mean Difference (SMD) and random effects indicated that there was an increase in the wet weight of sputum during and after 1 hour of ACBT in comparison with the conventional physical therapy approach, the use of external oscillatory devices and the control. It showed that the body of evidence was categorized as good and of high level. After assessing the variable of risk of bias, the research evidences favored ACBT over the conventional and alternative short terms in terms of secretion clearance13 ACBT when used with Forced Expiratory Technique (FET) can improve airway clearance14 and shows better radiographic clearing, which further reduces hospital stay15, therefore, this study is focused on observing their combined effect with early mobilization.
Significance Of Study: It is imperative to measure the consequences of mobilization on the respiratory and hemodynamic parameters of the ill obese patients in the Intensive Care Unit along with the effects of active cycle breathing techniques on to respiratory parameters and once the response of the mobilization and ACBT was determined, it can then help with determining the best treatment option for the patients who are critically ill and obese.
Objectives Of Study: To determine the combined effects of Active Cycle Breathing Techniques and early mobilization on the hemodynamic & respiratory responses of Obese Patients in Intensive care unit.
MATERIALS AND METHODS
Study Design: Randomized controlled trial.
Setting: ICU patients at Railway Hospital, Rawalpindi and Policlinic hospital Islamabad.
Duration of Study: 6 Months (1 January 2017 to 30 June 2017).
Sample Size: 29 patients in each group.
Sampling Technique: Purposive non-Probability Sampling technique was used and randomly assigned by coin toss methods.
Mobilization Protocol: Given below are the standards that were considered as intolerance findings:
| • | 20 mmHg rise or fall in the systolic blood pressure (SBP) or the diastolic blood pressure (DPB). |
| • | A rise of fall in the heart rate (HR) 20 beats/minute. |
| • | Peripheral capillary oxygen saturation, SpO2< 90%. |
| • | Syncope, faintness, paradoxical breathing, dizziness, and excessive perspiration16. |
Sample Selection:
| Table 1: Sample selection criteria | |
| Inclusion criteria: | Exclusion criteria: |
| 1.Hemodynamic Stability | 1.BMI<30, |
| 2.GCS >13, absence of anemia, | 2.Hemodynamically unstable patients, |
| 3.Respiratory and metabolic problems, | 3.Patients having septic shock |
| 4.No agitation, | 4.Massive blood loss, |
| 5.(BMI is 30 or over) | 5.Multiple trauma, |
| 6.Obese ICU patients, | 6.High risk surgery, |
| 7.Confused or high-risk patients | |
Subjects were given the consent form and the purpose of the research and consent was explained to the subjects verbally.
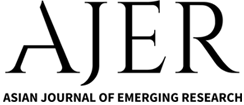
Data Collection Procedure: Two groups were selected by purposive non-probability sampling technique. Groups were controlled and experimental group. Patients in controlled group were given treatment of mobility in ICU as per patient’s tolerance, total session time was of 20-30 minutes, given thrice/day. Patients in the experimental group were given treatment of mobility in ICU as per tolerance along with the ACBT’s, with total session time of 20-30 minutes, thrice a day. ACBT’s treatment used in experimental group comprised 2-3 repetitions with 3 sessions per day. The patient’s blood pressure, temperature, respiration rate, pulse, Sp02, and rate of perceived exertion, FEV1/FVC will be taken at base line and after the treatment, as shown in Consort flow diagram (Figure 1).
Data Collection Tools:
- Self-structure questionnaire
- Borg’s scale17,18
- Clinical Spirometer
- Pulse oximeter
- Sphygmomanometer
- ICU mobility scale19
Self Structure Questionnaire: A simple form comprised of the demographical data of the patients, along with their personal history of smoking, diabetic profile, socioeconomic status as well as Glasgow Coma Scale level and body mass index along with the record of baseline vitals (pulse rate (PR), SpO2, Blood pressure (BP) and respiration rate (RR)) was used. The second half of the form consisted of the records of the pre-treatment and post-treatment values of BP, temperature, RR, PR, SPO2, rate of perceived exertion (RPE), FEV1, FVC, PEF, FEV1/FVC, ICU mobility scale score, treatment method & time.
Data Analysis Procedure: All the patients in the study were evaluated at baseline before the application of intervention. Data was then analyzed by IBM SPSS 21 (statistical package for social science) and later expressed in the form of table, charts and graphs.
RESULTS
Below are some of the important P values obtained by the statistical analysis of the results obtained.| Table 2: P values obtained by Friedman Test | ||
| P Value | ||
| Variables | Experimental Group | Control Group |
| Respiratory Rate | 0.000* | 0.637 |
| Pulse Rate | 0.009* | 0.016 |
| SpO2 | 0.009* | 0.016 |
| FEV1 | 0.000* | 0.012 |
| FVC | 0.000* | 0.476 |
| PEF | 0.000* | 0.188 |
| * Significant P value | ||
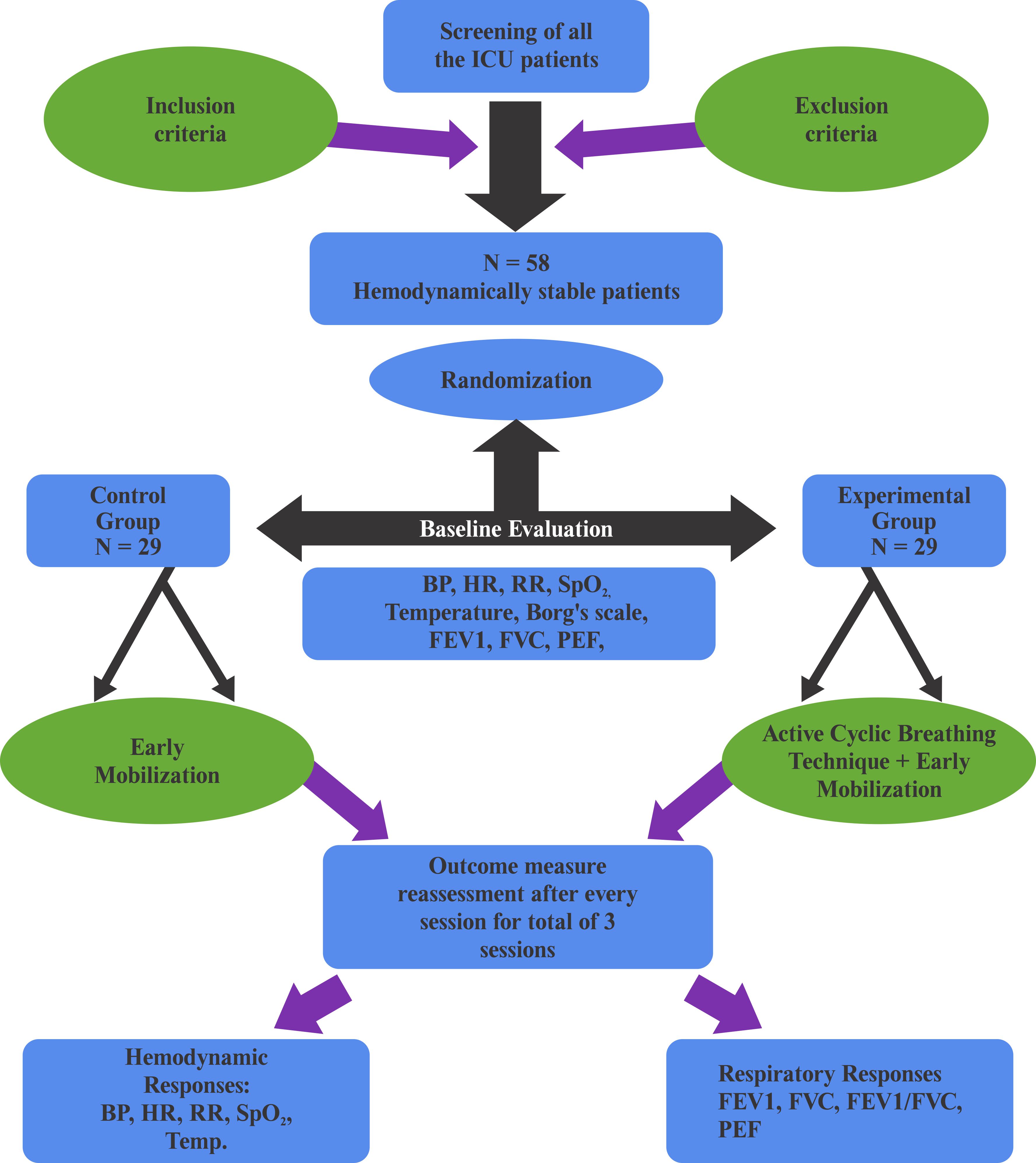
Marked improvement in Respiratory parameters: There has been progress in the values of FEV1, FVC and PEF in the experimental group over the control group, which means that the combination of ACBT with mobility training has positive effect on the spirometric values of the patient, it is statistically proved by having significant P value as shown in table 2 above. It is important to note here that the better values are observed by the end of third session as shown in the bar graphs below, where Wilcoxon test is applied for within group parameter of individual variable.
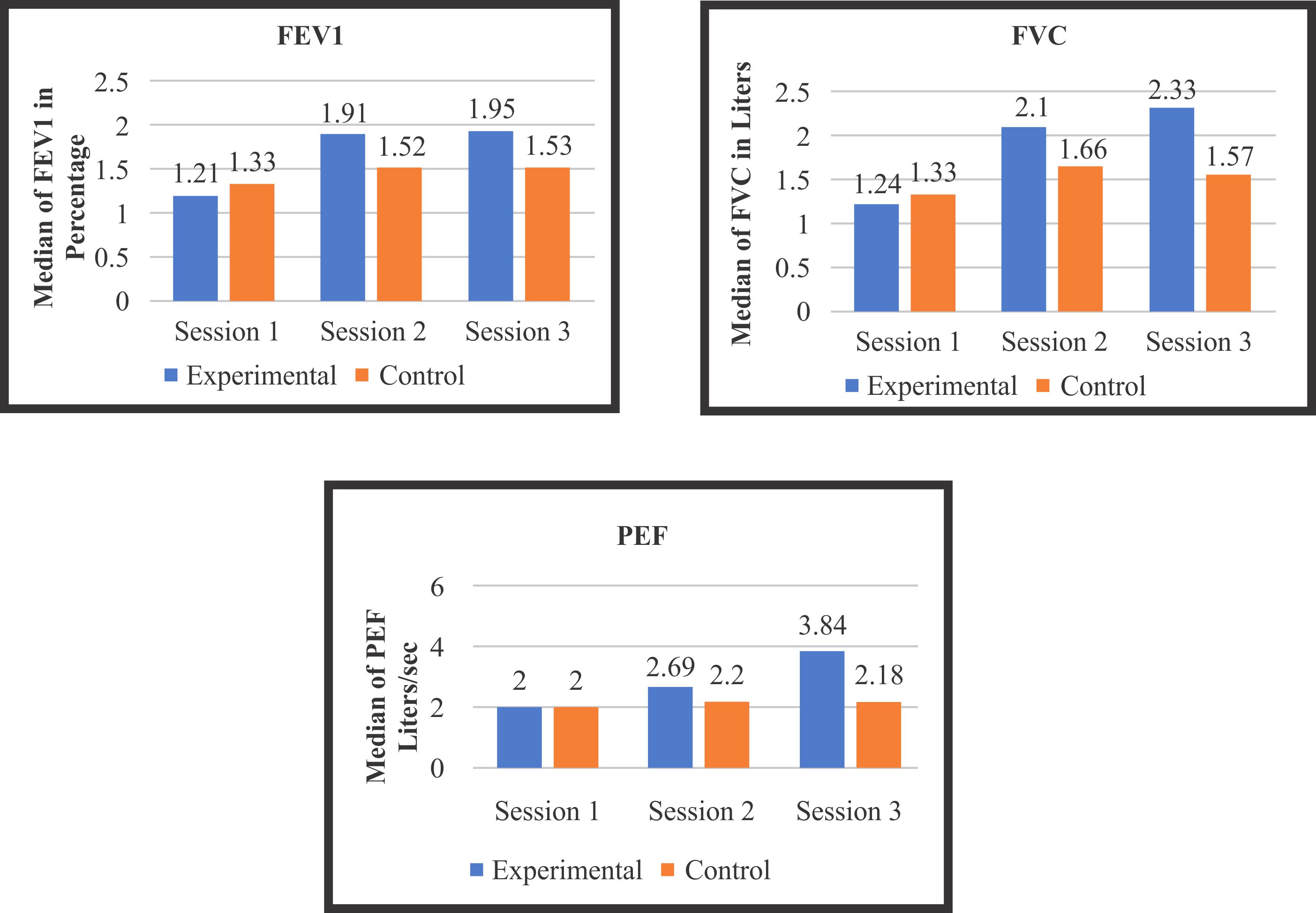
Noticeable decrease in the Pulse Rate & Respiration rate (Hemodynamic Parameter): In Experimental group, slight decrease in pulse rate and respiration rate, that remain almost consistent with the 3 sessions, as shown in graph below. Though the difference is not very marked in the respiratory rate, but it could be due to the fact that the sample size was not too big. Statistically significant P value as shown in Table 2 implies that ACBT with mobilization is effective for improving respiratory parameters.
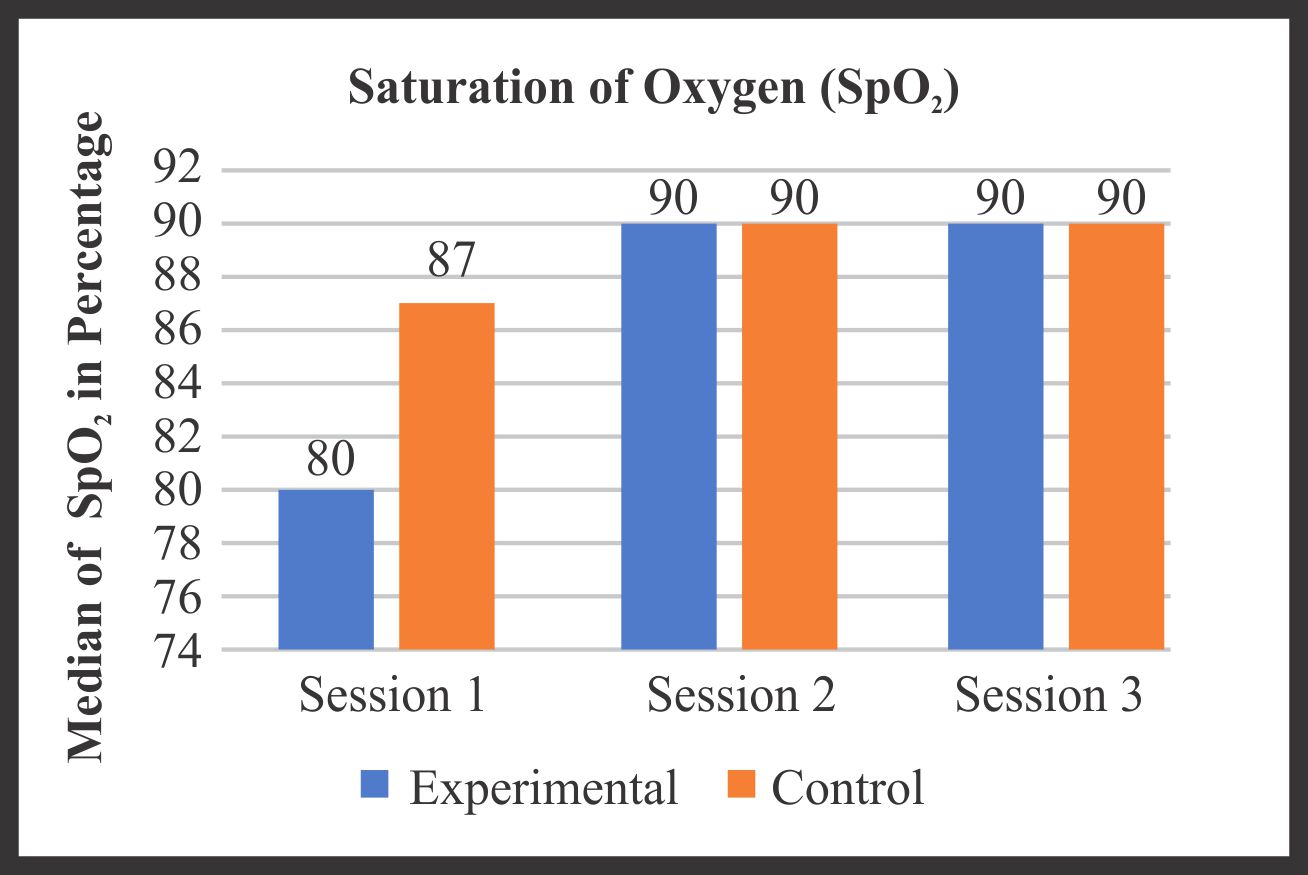
Analysis of SpO2: Peripheral capillary oxygen saturation has been improved significantly in comparison of the 3rd session with the 1st but the control group also shows similar effects. Therefore both mobilization alone and ACBT with mobilization are effective to improve oxygen saturation in the patients as shown in the graph below. It is proved statistically by Friedman test in the Table 1 above.
DISCUSSION
One of the study discussed in the meta analysis done by Lewis was of Milne SM, Eales CJ which showed that there was improvement in the values of FEV1 from base line post ACBT ( from 1.23 to 1.34) while that in FVC it was 2.85 to 2.98, that of in the ratio of FEV1/FVC it showed improvement from 45.62 to 47.55 and in case of PEF the values at baseline and that of Post ACBT were 4.44 and 4.7 respectively13. This study supports the results of researcher’s current study which showed that there had been improvement in the values of FEV1, FVC, ratio of FEV1/FVC and PEF in the experimental group over the control group. One similarly noted is that the difference had been marked in the third session as shown by the Graph 1.The above findings of the study have been supported by the work of Shiraz et al.20 in year 2015 who studied the effects of ACBT on 100 COPD patients with respect to their blood gases and oxygen saturation and came to the conclusion that there has been rise in the respiration rate with significant fall in the heart rate post treatment in the experimental group. The results of their study somewhat support the current findings of this study (Graph 2). Although the difference is not very marked, but statistically the P-value is significant (Table 2). It means that cardiac and respiratory reserve significantly increase using ACBT along with mobilization.
Stiller et al.21 observed the safety of mobilization and its effects on hemodynamic status and respiratory parameters in the ICU and found out that cardiac and respiratory reserves (HR, BP) significantly increase during and after mobilization21 similar to the outcomes of current study (Table 2)
Similarly the study of Shiraz et al.20 showed marked improvement in the value of SpO2 in the experimental group where ACBT was done on the patients. These findings back the findings of the current study as depicted in Graph 3.
Paneeth et al.22 conducted a randomized controlled trial on 30 patients with bronchiectasis and treated one group with ACBT and another with postural drainage. Their results showed that the not only does ACBT positively affect airway clearance, but has also improved FVC, FEV1 and SPO2, as proved in the current study in the form of graphs 1 and 3 respectively.
Shingavi et al.23 studied the effects of ACBT and autogenic drainage in patients with abdominal surgery and concluded that ACBT is more effective for increasing/improving chest expansion and inspiratory capacities in patients who had abdominal surgery. Though most of the patients with such surgery usually are transferred to ICU first so the results of our study on ICU patients out of which some had undergone abdominal surgeries due to obesity showed improvement in inspiratory capacities Graph 1.
As per a Cochrane review by Osadnik, published on March 201215, 28 studies comprising of 907 participants showed that the use of airway clearance techniques like ACBT was associated with very significant short term decline in the escalated requirement for the ventilator assistance. Along with other factors, one of the reason is improved SpO2 post ACBT, which supports the current findings of this study as shown in the Graph 3 above. Another study conducted on the same review15 proved that there has been much reduced long term need for hospitalization with benefits on the future flare-up episodes and the quality of life by early ACBT.
CONCLUSION
The study concluded that there has been a positive effect of Active Cycle Breathing Technique and early mobilization combined on the respiratory and some hemodynamic responses of ill obese patients in the Intensive Care Unit, It can not only reduce the complications of the illness but can positively affect the cardiac and respiratory reserves, thus helping in better recovery and good prognosis. It can also reduce the length of hospital stay, thus reducing the cost of illness.REFERENCES
- Lewis, L.K., M.T. Williams and T.S. Olds, 2012. The active cycle of breathing technique: A systematic review and meta-analysis. Respirat. Med., 106: 155-172.
- Hodgson, C.L., S. Berney, M. Harrold, M. Saxena and R. Bellomo, 2013. Clinical review: Early patient mobilization in the ICU. Critical Care.
- Dattani, R.S., C.B. Swerner, J.R. Stradling and A.R. Manuel, 2016. Exploratory study into the effect of abdominal mass loading on airways resistance and ventilatory failure. BMJ Open Respirat. Res.
- Stommel, M. and C.A. Schoenborn, 2009. Accuracy and usefulness of BMI measures based on self-reported weight and height: Findings from the NHANES & NHIS 2001-2006. BMC Public Health.
- Skinner, E.H., K.J. Haines, S. Berney, S. Warrillow, M. Harrold and L. Denehy, 2015. Usual care physiotherapy during acute hospitalization in subjects admitted to the ICU: An observational cohort study. Respirat. Care, 60: 1476-1485.
- Dambaugh, L.A. and M.M. Ecklund, 2016. Progressive care of obese patients. Crit. Care Nurse, 36: 58-63.
- The World Bank Group, 2019. Pakistan.
- Mendis, S., T. Armstrong, D. Bettcher, F. Branca and J. Lauer et al., 2014. Global Status Report on Noncommunicable Diseases 2014. World Health Organization, Geneva.
- Bach, P.B., C. Brown, S.E. Gelfand and D.C. McCrory, 2001. Management of acute exacerbations of chronic obstructive pulmonary disease: A summary and appraisal of published evidence. Ann. Internal Med., 134: 600-620.
- De Jonghe, B., J.C. Lacherade, T. Sharshar and H. Outin, 2009. Intensive care unit-acquired weakness: Risk factors and prevention. Crit. Care Med., 37: S309-S315.
- Gosselink, R., J. Bott, M. Connor, E. Dean and J.L. Vincent et al., 2008. Physiotherapy for adult patients with critical illness: Recommendations of the European Respiratory Society and European Society of Intensive Care Medicine Task Force on Physiotherapy for Critically Ill Patients. Intensive Care Med., 34: 1188-1199.
- Ciesla, N.D., 1996. Chest physical therapy for patients in the intensive care unit. Phys. Ther., 76: 609-625.
- Genc, A., S. Ozyurek, U. Koca and A. Gunerli, 2012. Respiratory and hemodynamic responses to mobilization of critically ill obese patients. Cardiopulm. Phys. Ther. J., 23: 14-18.
- Hollandl, A.E. and B.M. Buttonl, 2006. Is there a role for airway clearance techniques in chronic obstructive pulmonary disease? Chronic Respirat. Dis., 3: 83-91.
- Osadnik, C.R., C.F. McDonald, A.P. Jones and A.E. Holland, 2012. Airway clearance techniques for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev.
- Senduran, M., S.U. Yurdalan, D. Karadibak and A. Gunerli, 2010. Haemodynamic effects of physiotherapy programme in intensive care unit after liver transplantation. Disabil. Rehabilit., 32: 1461-1466.
- Chen, M.J., X. Fan and S.T. Moe, 2002. Criterion-related validity of the Borg ratings of perceived exertion scale in healthy individuals: A meta-analysis. J. Sports Sci., 20: 873-899.
- Pfeiffer, K.A., J.M. Pivarnik, C.J. Womack, M.J. Reeves and R.M. Malina, 2002. Reliability and validity of the Borg and OMNI rating of perceived exertion scales in adolescent girls. Med. Sci. Sports Exerc., 34: 2057-2061.
- Hodgson, C., D. Needham, K. Haines, M. Bailey and A. Ward et al., 2014. Feasibility and inter-rater reliability of the ICU mobility scale. Heart Lung, 43: 19-24.
- Sheraz, S., F.A. Siddiqi, S.A. Zaidi and I. Amjad, 2015. Blood gases and oxygen saturation response to active cycle of breathing techniques in COPD patients during phase I of cardiac rehabilitation. Rawal Med. J., 40: 259-262.
- Stiller, K., A. Phillips and P. Lambert, 2004. The safety of mobilisation and its effect on haemodynamic and respiratory status of intensive care patients. Physiother. Theory Pract., 20: 175-185.
- Puneeth, B., C.K.M. Faisal, D.M. Renuka and S. Ajith, 2012. Efficacy of active cycle of breathing technique and postural drainage in patients with bronchiectesis-A comparative study. J. Med. Health Sci., 2: 129-132.
- Shingavi, S.S., A. Kazi, S. Gunjal and M. Lamuvel, 2017. Effects of active cycle of breathing technique and autogenic drainage in patient with abdominal surgery. Int. J. Applied Res., 3: 373-376.
How to Cite this paper?
APA-7 Style
Fatima,
A., Ali,
R., Sharif,
S., Amjad,
I. (2019). Effects of ACBT with Early Mobilization on Respiratory/Hemodynamic Response of Obese ICU patients. Asian Journal of Emerging Research, 1(2), 98-105. https://doi.org/10.3923/AJERPK.2019.98.105
ACS Style
Fatima,
A.; Ali,
R.; Sharif,
S.; Amjad,
I. Effects of ACBT with Early Mobilization on Respiratory/Hemodynamic Response of Obese ICU patients. Asian J. Emerg. Res 2019, 1, 98-105. https://doi.org/10.3923/AJERPK.2019.98.105
AMA Style
Fatima
A, Ali
R, Sharif
S, Amjad
I. Effects of ACBT with Early Mobilization on Respiratory/Hemodynamic Response of Obese ICU patients. Asian Journal of Emerging Research. 2019; 1(2): 98-105. https://doi.org/10.3923/AJERPK.2019.98.105
Chicago/Turabian Style
Fatima, Abeer, Rabbi Ali, Saad Sharif, and Imran Amjad.
2019. "Effects of ACBT with Early Mobilization on Respiratory/Hemodynamic Response of Obese ICU patients" Asian Journal of Emerging Research 1, no. 2: 98-105. https://doi.org/10.3923/AJERPK.2019.98.105

This work is licensed under a Creative Commons Attribution 4.0 International License.